139 megapixel chip needed for retinal substitute
this article is from 2007 when cell phone cameras were not ubiquitous.
so what is the progress in the last 12 year ?
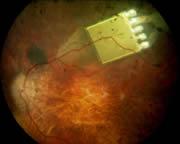
 The eyes have it: retinal implants could give sight back to people blinded by disease.© Punchstock
The eyes have it: retinal implants could give sight back to people blinded by disease.© Punchstock
this article is from 2007 when cell phone cameras were not ubiquitous.
so what is the progress in the last 12 year ?
Published online 21 March 2007 | Nature | doi:10.1038/news070319-7
News
A chip in the eye boosts sight
Amplification of light restores limited vision in some damaged retinas.
Retina Implant
The first test of an electrically boosted light-sensitive electronic chip implanted into the eye shows that it can restore sight to some blind patients.
This is another step in what is now a highly competitive — and commercial — global race to help the blind see again.
Eberhart Zrenner, executive director of the Eye Hospital at the University of Tübingen in Germany, announced at a recent press conference that his team had surgically implanted a 3-millimetre-square chip behind the retina of one eye in seven legally blind patients between the ages of 26 and 58. The chips restored limited vision to three of the patients, Zrenner said. The group will present its results at the Association for Research in Vision and Ophthalmology annual meeting in Fort Lauderdale, Florida, in May.
The chips were developed and made by Retina Implant of Reutlingen, Germany, a start-up company co-founded by Zrenner. Walter Wrobel, chief executive officer of the company, says they will now "fine tune" the chips and have them ready to market in 2009 at a price of €25,000 each. "We now know what improvements need to be made and we need more tests."
Broken retina
Research groups around the world are working on various type of implant designed to restore sight to people who have lost retinal function. Implants can work for conditions such as age-related macular degeneration or retinitis pigmentosa, but not for blindness caused by glaucoma or diabetes, among other conditions.
What distinguishes the Retina Implant from other sub-retinal devices is that it is powered by electricity to amplify the images, says Wrobel. The chip contains 1,500 light-sensitive microelectrodes, each generating a picture element (pixel), and each with an amplifier that boosts the signal delivered to stimulate the retina. The device is implanted in a five-hour operation, with a wire running out of the eye socket, under the skin, to behind the patient's ear. This is then connected to a power source.
For two of the patients who showed no improvement in the trial there were technical problems with the chips; two others had been blind for more than 10 years, and so seemed to have lost the ability to interpret the light signals.
The three patients in whom the chip worked reported seeing "sort of an illuminated window frame", in which they had limited vision. One was able to locate white dinner plates on a dark tablecloth, for example, but could not locate white plastic packages of coffee creamer.
"The patients were absolutely enthusiastic about it, to see light or find a plate on the table in front of them," says Wrobel. "For them, it was tremendous progress." A key to future success will be teaching patients to interpret the images better, he says.
Long-term effects of the implants are not yet known: six of the seven patients carried the implant for 30 days, after which it was surgically removed. The seventh patient carried the chip for 18 months with no complaints.
Tough competition
The German project is just one among many aiming to fix faulty retinas. Alan Chow at Rush University Medical Center in Chicago is a co-founder of Optobionics of Naperville, Illinois. His team has a sub-retinal implant that works without amplification, and is powered only by the incoming light. "We have demonstrated that a passive device works," Chow says, adding: "With ours there is no need for an exit wire."
An artificial silicon retina developed by Optobionics, with 5,000 microscopic solar cells, each with its own stimulating electrode, has been tested in ten people in a trial that began in 2000. The company says that sight improved for all of them. Chow says some have seen colours and others have been able to see their own face in a mirror. But Wrobel still argues that amplification is necessary to truly restore sight.
Yet another group, led by the Doheny Eye Institute at the University of Southern California in Los Angeles, is working on an implant that requires the patient to wear a tiny camera and microprocessor mounted in eyeglasses, along with an implant, a receiver and a battery pack.
ADVERTISEMENT
A device developed by Second Sight, a company involved with the Doheny project, has been in human trials since 2002. The first generation of these implants enabled a formerly blind patient to distinguish between objects on a table and make out large letters (see 'Artificial retina gets diamond coating'). A new device with more pixels is set to be tested soon, the team reported at the recent meeting of the American Association for the Advancement of Science in San Francisco.
But some say the small camera is clunky and intrusive. "I do not see this as practical," Wrobel says.
Brian Mech, senior director of business development at Second Sight, says Retina Implant has not presented much data publicly, making it difficult to comment on any advantages this system may offer.
Visit our chipintheeyeboostssight.html">newsblog to read and post comments about this story.
Artificial retina gets diamond coating
Nanofilm will protect electronic implant.
The eyes have it: retinal implants could give sight back to people blinded by disease.© Punchstock
A bionic eye that allows blind people to see has now got a protective coat of diamond that should significantly improve its performance.
The silicon chip retinal implant is being developed by Second Sight, a company based in Sylmar, California, along with a consortium of university researchers. The device needs a hermetic case to prevent it from reacting with fluids in the eye.
"It's as if you're throwing a television into the ocean and expecting it to work," says the company's president, Robert Greenberg. "The approach until now has been to lock it in a big waterproof can, but it's very big and bulky," he explains.
So researchers have developed an ultrananocrystalline diamond (UNCD) film that is guaranteed to be safe, long-lasting, electrically insulating and extremely tough. The coating can also be applied at low temperatures that do not melt the chip's microscopic circuits.
“It's as if you're throwing a television into the ocean and expecting it to work.”
The UNCD film is the first coating to meet all the necessary criteria for the implant, says Xingcheng Xiao, a materials scientist at Argonne National Laboratory, Illinois, who developed the film.
The tiny diamond grains that make up the film are about 5 millionths of a millimetre across. They grow from a mixture of methane, argon and hydrogen passing over the surface of the five-millimetre-square chip at about 400 °C. Xiao and his colleagues have already tested the implants in rabbits' eyes, and saw no adverse reaction after six months. He will present the results on 1 April at the Materials Research Society meeting in San Francisco, California.
Lighter load
A healthy retina contains rod and cone cells that convert light into electrical impulses, which fly to the brain through the optic nerve. But for millions of people with diseases such as retinitis pigmentosa or macular degeneration, these cells do not work properly.
The retinal implant bypasses these diseased cells by electrically stimulating healthy cells that sit beneath them at the back of the eyeball. The patient 'sees' using a pair of glasses carrying a tiny video camera that sends digitized images to the implant using radio waves.
The first human trial of Second Sight's artificial retina has been running since 2002, and it has enabled a formerly blind patient to distinguish between objects such as cups and plates, and even to make out large letters. But with only 16 electrodes, the device does not allow the patient to see a clear picture. For that, thousands of electrodes are needed on the same size of chip, making it even more delicate.
ADVERTISEMENT
In the first trial, the electronics package was separated from the electrodes and implanted behind the patient's ear because its casing was so bulky, explains Greenberg. The team's goal is to integrate everything into a single unit that fits neatly into the eye. Xiao adds that a UNCD coating could be equally useful for other implantable devices, such as biosensors to monitor a patient's health.
"They've managed to create a diamond film that is of considerably higher quality than other methods have managed," says Doug Shire, a materials engineer at Cornell University in Ithaca, New York, who is part of the Boston Retinal Implant Project. "But the ultimate potential of these devices will only be told in long-term trials," he adds.
Second Sight is planning clinical trials of a 60-electrode device this year, but it may be several more years before the diamond-coated chip is used in humans, says Greenberg.
President of Second Sigh
