The poor and lack of disease and cancer registry implementation in India
When I joined pediatric surgery fellowship Niloufer Institute of Maternal and Child Health (located in Hyderabad presently in the Telangana state)
it's
my professor asked me to maintain a cancer registry of pediatric cancers we were operating upon and at that time I did not know anything about cancer so I requisitioned a large accounting register's and wrote down in longhand the various demographic details and the operating procedures and the minimal pathological results we used to get in those times.
After coming to USA I have changed careers and have become an general internal physician and have lost touch with pediatric surgery except an occasional foray into nostalgia and an occasional interesting pediatric surgical article.
Recently a person close to me was diagnosed with cancer and I have been doing some reading up and one thing which struck me was the detailed cancer registries maintained by multiple organizations in USA/
I could hardly get any good information regarding registry maintenance and the various institutes in India.
When I joined pediatric surgery fellowship Niloufer Institute of Maternal and Child Health (located in Hyderabad presently in the Telangana state)
it's
my professor asked me to maintain a cancer registry of pediatric cancers we were operating upon and at that time I did not know anything about cancer so I requisitioned a large accounting register's and wrote down in longhand the various demographic details and the operating procedures and the minimal pathological results we used to get in those times.
After coming to USA I have changed careers and have become an general internal physician and have lost touch with pediatric surgery except an occasional foray into nostalgia and an occasional interesting pediatric surgical article.
Recently a person close to me was diagnosed with cancer and I have been doing some reading up and one thing which struck me was the detailed cancer registries maintained by multiple organizations in USA/
I could hardly get any good information regarding registry maintenance and the various institutes in India.
Registry Plus™ Software Programs for Cancer Registries
Registry Plus is a suite of publicly available free software programs for collecting and processing cancer registry data. The Registry Plus suite can be used separately or together for routine or special data collection. These software programs, compliant with national standards, are made available by CDC to implement the National Program of Cancer Registries, established by Public Law 102-515.
Registry Plus Components
Also Available
- Registry Plus Computer Systems and Personnel Requirements [PDF-409KB]
- Registry Plus Suite Data Flow Diagram [PDF-49KB]
- Policy and Letter of Agreement for Use of CDC-Developed Software by Users External to the National Program of Cancer Registries [PDF-13KB]
- Royalty-free License
- Frequently Asked Questions
- Hardware Requirements and Technical Support
Suggested Citation
Registry Plus, a suite of publicly available software programs for collecting and processing cancer registry data. Atlanta (GA): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion; 2015. Available at: https://www.cdc.gov/cancer/npcr/. Accessed month/day/year.
Cancer Registration & Surveillance Modules
The Cancer Registration & Surveillance modules provide information needed by cancer registry staff and others interested in collecting and recording the most complete and accurate cancer data possible. The modules cover information on:
- Registries and their operations
- Basic anatomy and medical terminology
- Cancer tests and treatments
- Coding and staging standards for cancer registration
- Casefinding and follow-up
Note: The following modules have moved from the Cancer Registration and Surveillance Modules to the References section: Introduction to Collaborative Stage, ICD-O-3, and Summary Stage 2000.
Cancer Registration
The Cancer Registration module introduces you to the basic concepts related to cancer registration, the different types of cancer registries, the importance of collecting cancer data, and the process of its collection.
In this module you will learn how to:
- Define key concepts related to cancer registration.
- Describe the history of cancer registration.
- Explain the importance of cancer registration in fighting cancer.
- Name the two major types of cancer registries and describe how they differ.
- List the four major cancer data categories.
- Describe the cancer data collection process.
- Explain the importance of patient confidentiality and how it is protected.
Cancer Registry
Cancer data is important to many people for a variety of different reasons. Researchers need accurate, up-to-date cancer data to study possible causes of cancer. Medical administrators use cancer data to make decisions regarding equipment purchases and developing programs for cancer prevention. Departments of Health use cancer data to investigate potential cancer clusters and their causes. Some of the data are available on the Internet without effort while other data can only be accessed with special permission. Where does the data come from and how is it collected?
In fact, all these valuable cancer statistics are collected and provided by the cancer registry.
By definition, a cancer registry is an information system designed for the collection, storage, management, and analysis of data on persons with cancer, usually covering a hospital or group of hospitals.
A cancer registry is a particular type of disease registry and its major purposes are:
- to establish and maintain a cancer incidence reporting system;
- to be an informational resource for the investigation of cancer and its causes; and
- to provide information to assist public health officials and agencies in the planning and evaluation of cancer prevention and cancer control programs.
Cancer registries are a primary source for unbiased population-based case control studies, the end points for cohort studies and clinical trials -- and perhaps most importantly, the beginning point for survival analysis.
Cancer registration refers to the process of continual, systematic collection of data on the occurrence and characteristics of reportable malignancies with the purpose of helping to assess and control the impact of cancer on the community. Behind this system is a group of hardworking people called cancer registrars who are trained to collect accurate,
Cancer Registrars
Cancer registrars are the data management experts who collect cancer data from a variety of sources and report the resulting cancer statistics to various healthcare agencies. The primary responsibility of the cancer registrar is to ensure that timely, accurate, and complete cancer data is collected and maintained on all types of cancer diagnosed and/or treated within an institution or other defined population. Information is entered into a computer database manually or through database linkages and computer interfaces.
Cancer registrars' work goes far beyond simply collecting cancer data. In order to accomplish the goal of preventing and controlling cancer, they also work closely with physicians, administrators, researchers, and health care planners to provide support for cancer program development, ensure compliance of reporting standards, and serve as a valuable resource for cancer information.
Cancer registrars bridge the information gap by capturing a complete summary of a patient's disease from diagnosis to death. The information included in the summary is not limited to the episodic information contained in the health care longitudinal record. Instead, the summary or abstract is an ongoing account of the cancer patient's history, diagnosis, treatment, current status, and outcome of treatment.
In the past, cancer registrars were trained primarily on the job. Today, however, formal education programs at colleges around the country teach cancer data management. Curricula include, but are not limited to, cancer and its management, medical terminology, anatomy and physiology, biostatistics and epidemiology, cancer data abstracting, database record management, cancer program management, and cancer registry procedures. In addition to formal college courses, training is available from programs that vary from one to two weeks in duration and provide an intensive training experience in cancer registry operations. Due to the revolution of the Internet, web-based training modules are also now becoming a viable cancer registrar training tool. By completing this series of online training modules, one may be inspired to pursue cancer registration as a profession.
Review: Cancer Registration
In Cancer Registration, we learned that the cancer registry is an information system established for the collection, storage management, and analysis of cancer data. Cancer registration refers to the process of continual, systematic collection of data on the occurrence and characteristics of reportable malignancies with the purpose of helping to assess and control the impact of cancer on the community. Behind the system are people, cancer registrars, who are responsible for collecting the cancer data and making sure they are timely, accurate, and complete.
A very brief history of cancer registration indicates that the recorded effort of collecting cancer-related data started in eighteenth century Europe, and the first hospital-based cancer registry came into being in New Haven, Connecticut.
Types of Registries
There are two major types of cancer registries: hospital-based registries and population-based registries. There are two sub-categories under hospital-based registries: single hospital registry and collective registry. Depending on the operators, population-based registries can be administrative, research, or cancer control oriented. Ideally, registries of a combination of above three functions predominate due to the mission of the primary funding source.
The goals of hospital-based registries include:
- Improvement of patient care
- Professional education
- Administrative information
- Clinical research
The goals of population-based registries are:
- Cancer prevention
- Early detection
- Determination of cancer rates and trends
- Patterns of care and outcomes
- Research
- Evaluation of control efforts
These two types of cancer registries will be discussed in detail in the following two sections.
There is another type of cancer registry: special cancer registry. These are cancer registries established to collect and maintain data on a particular type of cancer. For example, the Gilda Radner Familial Ovarian Cancer Registry is a special cancer registry that collects cancer information from those families with two or more relatives having ovarian cancer. Other special cancer registries exist that collect data on brain tumors, colorectal cancer, or lung cancer. These special cancer registries often provide educational opportunities for those who want to learn more about a particular type of cancer and support for those who may suffer from it.
is a special cancer registry that collects cancer information from those families with two or more relatives having ovarian cancer. Other special cancer registries exist that collect data on brain tumors, colorectal cancer, or lung cancer. These special cancer registries often provide educational opportunities for those who want to learn more about a particular type of cancer and support for those who may suffer from it.
is a special cancer registry that collects cancer information from those families with two or more relatives having ovarian cancer. Other special cancer registries exist that collect data on brain tumors, colorectal cancer, or lung cancer. These special cancer registries often provide educational opportunities for those who want to learn more about a particular type of cancer and support for those who may suffer from it.Hospital-Based Registries
Hospital-based cancer registries maintain data on all patients diagnosed and/or treated for cancer at a particular facility. The focus of the hospital-based cancer registry is on clinical care and hospital administration. If you have taken a look at the brief history of cancer registries on the previous page, you may have noticed that the first cancer registry in the United States, Yale-New Haven Hospital Cancer Registry, was a hospital-based registry.
There are two sub-categories under hospital-based registries: single hospital registries and multi-institution registries. The primary goal of the single hospital (institution) registry is to improve patient care by medical audit-type evaluation of outcomes. Cancer data collected by the single hospital (institution) registry are also used for physician education, as a source of data for some types of research, and for some facility utilization assessment.
On the other hand, the primary goal of collective registries (multi-institution registries) is to improve patient care by supporting institutional registries with common standards and pooled data. They often seek to establish the natural history and etiology of the reported cancers.
Population-based registries record all new cases in a defined population (most frequently a geographical area such as a state) with an emphasis on epidemiology and public health. In contrast to hospital-based registries, population-based registries are designed to determine cancer patterns among various populations or sub-populations, to monitor cancer trends over time, to guide planning and evaluation of cancer control efforts, to help prioritize health resource allocations, and to advance clinical, epidemiological, and health services research.
Population-Based Registries
In comparison to the hospital-based cancer registry, the data collected by the population-based registry serves a wider range of purposes.
Advantages of a population-based cancer registry include cancer control programs, patient care programs, administrative programs, and cancer research programs.
Data from population-based registries can be used for monitoring the distribution of late-diagnosed cases of cancer of the types for which early diagnosis is the strategy for control, esp., communities, ethnicities, age and other demographic groups.
For example, Cancer surveillance programs such as SEER (Surveillance, Epidemiology, and End Results) use cancer statistics collected by population-based registries to monitor the distribution of cases of cancer among certain occupations, communities, ethnicities, ages, and other demographic groups.
The population-based registry plays an important role in improving patient care programs. Linkage services from this type of cancer registry for care providers provide a cost-effective source of data necessary for clinical program, such as follow-up results of a mammography program, stage of diagnosis data to managed care organizations, treatment selection data for groups monitoring clinical treatment guidelines utilization, etc.
The cancer registry may also provide services to hospital cancer programs such as shared follow-up, death clearance, and pooled data on treatment, stage, or survival.
Many cancer agencies and organizations rely on data collected by population-based registries. Based on accurate and timely cancer statistics, healthcare planners make decisions on resource allocation, such as the placement of radiotherapy facilities, proper staffing of cancer control programs, and "market share" reports for existing facilities. Cancer statistics provided by population-based cancer registries make it possible for public health administrators to evaluate suspected clusters of cancer within communities or population groups.
Cancer research programs benefit greatly from the cancer data collected by population-based cancer registries: an unbiased group of cases can be selected for cancer studies; studies of association of cancer and other diseases, environments, occupations, or other sources of exposures
Review: Types of Registries
Types of Registries has provided you with information about the existing types of cancer registries, including population-based cancer registries, hospital-based cancer registries, and special cancer registries.
You have learned that the population-based registry has some advantages over other types because it serves a wider range of purposes. Data collected by population-based registries are used by physicians, researchers, medical students, and health care administrators alike. Research can be conducted based on an unbiased group of cases. In addition, using data collected from population-based cancer registries, cancer control agencies and programs make important decisions regarding the allocation of resources and prevention strategies.
Data Collection
The information collected by cancer registries can be placed into four categories: patient demographics, tumor (cancer) identification, treatment, and outcome.
Demographic data consists of the personal information about a patient such as the patient's name, age, gender, race, ethnicity, birthplace residence, etc. This information individually identifies the cancer patient. Without individual identifiers to check for duplicate registrations, the data would be inaccurate and unsuitable for analysis.
Cancer information results from the diagnostic findings about a patient. It includes the primary site of the malignancy, its cell type, and the extent of disease. Dates and results of procedures used to diagnose cancer are also recorded.
Data collection continues after a patient is diagnosed with cancer. Information regarding cancer treatment are also recorded (surgery, radiation therapy, chemotherapy, hormone, immunotherapy, and other).
Cancer registries continue to gather data after the cancer patient has received treatment. This data consists of information concerning the outcome of the treatment. Patient status is updated regularly to maintain accurate surveillance information. Lifetime follow-up on patients permits registries to record information about patient survival.
Process of Cancer Data Collection
Cancer data collection begins by identifying people with cancer who have been diagnosed or received medical care in hospitals, outpatient clinics, radiology departments, doctors' offices, laboratories, surgical centers, or from other providers who diagnose or treat cancer patients.
By law, these facilities are required to report new cancer cases to a central cancer registry such as a state cancer registry. The cases can be reported to the cancer registry electronically or in traditional paper format following nationally recognized reporting protocols to assure consistency in case reporting from facility to facility.
Cancer registries do not simply wait for cancer information to be handed over from the sources mentioned above. Instead, staff members of cancer registries become actively involved in casefinding activities so that the cancer information they receive is as complete as possible. Cancer registrars often accomplish this by visiting hospitals and clinics to ensure that no cancer data or cases are missed.
To ensure the quality of cancer data, cancer registries may create and adopt their own innovative data collection systems. For example, the New Hampshire Cancer Registry utilizes a two-phase reporting system, which requires that cancer information (primary site, histology, etc.) be reported within 95 days of diagnosis and demographic and staging information be reported within 180 days of the date of diagnosis.
Cancer data collection is a time- and labor-intensive effort, but the great value of its product, cancer statistics, makes all of the hard work worthwhile.
Confidentiality
Cancer data are highly confidential. Improper disclosure of these data could result in emotional, psychological, and financial harm to patients and their families. Therefore, one of the most important responsibilities of cancer registry professionals is to protect the confidentiality of cancer patient information.
At the state level, legislative efforts have been made to improve and protect the confidentiality of cancer data. Specific regulations and laws determine to whom cancer information may be reported, how cancer information is reported, and what procedures should be taken to access cancer information. For example, information identifying a patient is removed when the data is reported. In addition, researchers who need access to cancer data must receive special permission from a designated authority. Each cancer registry may have its own strict policy regarding the way in which files and documents containing confidential information are handled. As a result of such policies and procedures, the privacy of cancer patients is protected.
There are also federal standards to protect the privacy of individually identifiable health information. These standards are included in the HIPAA (the Health Insurance Portability and Accountability Act of 1996) regulations. View the Standards for Privacy of Individually Identifiable Health Information.
Although patient confidentiality is of paramount importance, cancer registries also may implement policies to protect the privacy of physicians and health care facilities.
Review: Data Collection
- What data are collected?
- How are data collected?
- How are data handled?
You have learned that cancer data collected by cancer registries can be put into four categories: demographic, tumor (cancer) identification, treatment, and outcome (follow-up). The demographic information identifies the cancer patient; the cancer information identifies the malignancy; the treatment information is about the various options selected to treat the cancer patient; and the outcome information consists of detailed information after the cancer diagnosis and treatment such as the cancer status and the patient's vital status.
You have also learned how cancer data are collected. The process begins with the diagnosis of cancer. In most cases, the data collection does not end until the patient dies. Although facilities that accept and treat cancer patients may be required by law to report cases and provide cancer data to a central cancer registry, cancer registrars also go out and visit hospitals and clinics to collect timely and quality cancer information.
To protect privacy and confidentiality of cancer patients, physicians, and health care facilities, relevant regulations, policies, and laws are strictly implemented to guide the handling of information in cancer registries.
Cancer Registry Operations & Procedures
The Cancer Registry Operations & Procedures module provides you with the basic information about how cancer registries function. You will learn about the positions available in registries and the procedures for handling the data. In this module you will learn how to:
- Describe various cancer registry positions.
- Explain the factors that affect registry staffing.
- Explain why CoC-approved cancer programs must develop and maintain procedures manuals.
- Describe how the reference date is set.
- Define a reportable list and name the organization responsible for its development.
- Define data standards are and explain their importance.
- Name some of the organizations involved in determining data standards.
- Define data sets and explain how different requirements of standard setters can affect their elements and formats.
- Explain why standard code categories must meet multiple data goals.
- Explain why both technical and non-technical elements must follow rules for code category assignment.
- Describe how data edits affect the data quality.
- Describe how code category, assignment and data editing are related to case consolidation.
- Describe the basic data ma
Cancer Registry Management
Cancer registry supervisors have varying educational backgrounds. Although management styles also vary, successful management requires careful planning. This unit addresses several components that must be in place before the cancer registry begins to collect data. Unless otherwise specified, the term supervisor refers to any individual directly responsible for overseeing daily cancer registry operations.Cancer Registry Planning
The first step in the planning process is to define the registry's objectives. Once objectives are defined, personnel, space, and equipment can be determined. The Standards of the Commission on Cancer, Vol. I: Cancer Program Standards and Vol. II: Registry Operations and Data Standards (ROADS), provide a basis for objective development by outlining all requirements that must be met to attain approval. In addition, medical and administrative staff may contribute suggestions for additional objectives, depending on the goals of the institution.Although the majority of registry data are utilized by medical staff to evaluate cancer caseloads, treatment, and survival, some administrators are increasingly using registry data for resource planning and referral pattern identification. With the emergence of managed care, registry data may be used to identify service areas, physician recruitment opportunities, service usage, hospice needs, resource usage, or payment sources. As a result, the registry may need to modify objectives to meet changing institutional goals. Once defined, objectives provide a basis for developing registry staff position descriptions.Cancer Registry Position Descriptions
Cancer registry position descriptions should be specific enough to outline all job responsibilities, yet flexible enough to allow for the growth of both the staff and cancer program. Many facilities have specific formats for position descriptions. Although the formats may differ, position descriptions in all facilities should contain similar information. A registry position description should include requirements or comments regarding fourteen areas of responsibility, as shown in Table A. In smaller registries, one person may be responsible for all functions, in which case one position description covers all responsibilities. However, larger registries may require the development of several specialized position descriptions (for example, one for the cancer program manager, who handles administrative and staffing issues; another for abstractors, who abstract and code the data; and another for a follow-up person, who conducts all follow-up activities). Specialized position descriptions are more efficient and cost effective and cover a broader range of expertise and services.Cancer registry responsibilities may change with yearly caseloads or as cancer program responsibilities change. As a result, position descriptions should be reviewed and revised annually. Once cancer registry responsibilities are defined, staffing and workload distributions can be determined.Office Management
Planning is necessary to ensure that hospital or institution-based registry staffing meets the requirements of the Commission on Cancer (CoC) of the American College of Surgeons, and population-based registries meet the requirements of their funding agencies. Several factors affect registry staffing, including yearly caseload, data usage, longevity of the database, and managerial and administrative responsibilities, computerization, and cancer program functions. Institutions may hire part time or full time staff or consultants to perform registry and/or cancer program functions. The hours of cancer registry operations may vary. However, staff should be available during normal business hours to accommodate study requests from medical research and administrative staff. Staffing hours may also vary in order to facilitate follow-up calls to patients, outside institutions, or physician's offices. Methods for task distribution vary from registry to registry.The possibility of distributing and sharing responsibilities is greater in larger registries. Some registries delegate specific responsibilities to each staff member, whereas others distribute all responsibilities equally among all staff members. Abstracting responsibilities might be distributed by cancer site or alphabet. For example, a particular staff member may be responsible for abstracting and following all patients with breast cancer whose last names start with the letters A through D, and so on. Varying staff or their responsibilities allows the supervisor to achieve goals while providing staff with the opportunity to expand their knowledge and skills.Once data collection begins, continuous monitoring is necessary to ensure compliance with CoC and other agencies. For example, abstracting should be initiated between four and six months after diagnosis and the follow-up percentage must be maintained at required rates. When backlogs occur, rearranging responsibilities to meet deadlines may be necessary. The development of productivity standards will assist in maintaining compliance.Productivity Standards
Productivity standards should clearly define departmental and individual staff expectations, as well as performance and evaluation methods. The NCRA Registry Staffing Manual outlines specific productivity standards and suggestions for conducting time and motion studies for casefinding, abstracting, and follow-up. Conducting time and motion studies within the registry can help to establish internal productivity standards and/or validate existing standards. These standards provide a basis for performance evaluations by allowing measurement of job performance. In addition, productivity standards data can be used to justify the need for additional staff or equipment.Policy & Procedure Manual
Every registry should develop and maintain a policy and procedure manual that documents each phase of cancer registry operations. This manual promotes smooth operation of the registry and serves as a training reference for new staff. A complete and current procedure manual can help registry staff identify changes in the profession. Table B contains a list of items that should be included in a registry's policy and procedure manual.In addition to a a policy and procedure manual, computerized registries must also maintain an operations manual that addresses the items listed in Table C.The cancer committee or registry's governing body should be involved with the development of the policy and procedure manual. Once developed it should be reviewed and revised at least once a year. The procedure manual must be updated as procedures change to maintain current documentation.Reference Date
To ensure a valid statistical database, the Commission on Cancer (CoC) of the American College of Surgeons requires that a start date be established for CoC accredited registries. This date is known as the reference date. It should be set as January 1, of a given year. Once this date is established, all cases diagnosed and/or treated at the facility on or after this date must be entered into the registry. Registries in cancer programs seeking approval from the CoC must first accrue two years of data with one year of successful follow-up. The original reference date must be maintained unless one of the items in Table D occurs.Requests to change the reference date must be submitted in writing to the Commission on Cancer. They are considered and/or approved at the CoC's Cancer Department's administrative leveReportable List
The criteria for eligible cases in a registry depend upon the governing agencies of the registry. Along with state-specific reportable cases, registries participating in the Approvals Program of the Commission on Cancer (CoC) of the American College of Surgeons (ACoS) must use the reportable list defined by the CoC.The CoC requires the cancer registry to collect information on malignancies diagnosed and/or treated at the hospital, except for in-situ malignancies of the cervix and localized basal and squamous cell carcinomas of the skin. The cancer committee is responsible for developing a reportable list that identifies all types of cases to be included in the cancer registry database. The reportable list identifies malignancies with a behavior code (fifth digit) of 2 or 3 as identified in the International Classification of Diseases for Oncology, 3rd edition (ICD-O-3).In addition, the reportable list identifies reportable-by-agreement benign or borderline disease processes not required by the Commission on Cancer or state registries. These benign or borderline cases may be institution or registry-specific and mandated by the institution's cancer committee or governing board. Eligible basal, squamous, and basosquamous cell cancers of the skin should be identified. Ultimately, the reportable list includes malignant cases, reportable-by-agreement and diagnoses to be entered into the cancer registry database. A non-reportable case (diagnoses that should not be included) should also be maintained.The reportable list should be reviewed annually by the cancer committee or governing agency to determine the addition or deletion of reportable cases. When developing or changing the reportable list, it is important to remember that collecting additional reportable-by-agreement cases may necessitate additional staffing due to increased case load and related activities.Cancer Registry Organization
Cancer registry supervisory responsibilities vary depending on the size of the registry. In large registries, supervisors may spend more time monitoring and coordinating cancer program activities and staff. Supervisors in smaller registries may spend most of their time overseeing and performing registry functions.The department responsible for overseeing the cancer registry varies by institution. For example, the registry may be a part of medical oncology, radiation oncology, pathology, quality improvement services, health information management (HIM), or another appropriate department. In most instances, the registry supervisor reports to the director, assistant director, or administrator of the department. Inevitably, cancer registry operations are affected by the goals of the department overseeing it. For example, registry staff within the health information management (HIM) department may be used for coding, chart analysis, or chart retrieval when HIM backlogs or staffing shortages occur. Therefore, the administrator responsible for the cancer registry must be knowledgeable regarding registry purposes and functions. This is vital to ensure that adequate staffing and time are devoted to registry operations. The cancer committee is ultimately responsible for overseeing cancer registry operations. Educating cancer committee members regarding the functions of the registry is essential to ensure their support and guidance.Review: Cancer Registry Management
Here is what we have learned from this unit: - Cancer registry supervisors, with different educational backgrounds and management styles, are directly responsible for overseeing daily cancer registry operations.
- The Standards of the Commission on Cancer, Vol. I: Cancer Program Standards and Vol. II: Registry Operations and Data Standards (ROADS), provide a basis for objective development by outlining all requirements that must be met to attain approval.
- Cancer registry position descriptions should be specific enough to outline all job responsibilities, yet flexible enough to allow for staff and cancer program growth.
- Planning is required to ensure that registry staffing meets the requirements of the Commission on Cancer (CoC) of the American College of Surgeons.
- Productivity standards should clearly define departmental and individual staff expectations, as well as performance and evaluation methods.
- Every registry within a CoC-approved cancer program must develop and maintain a policy and procedure manual that documents each phase of cancer registry operations.
Data Standards
Standards are rules set by the governing authority. They reflect the organizational data needs of standard setters, including the need for consistency among groups. It is no accident that the history of oncology data standards is closely linked to groups that shaped their development. The standards that apply to cancer registries today evolved over the last century. The standard setters identified in this section established the principles of registry data and continue to influence cancer registry operations today. Their goals help determine what registries collect and how the data are processed and ultimately used. Within their spheres of responsibility, they are also the primary authorities to address questions on data and data management.Registry data collected in the absence of shared standards contribute little beyond anecdotal data towards case management or cancer control. Shared standards ensure clarity of communication, protect the integrity of data when pooled or compared across multiple sources, and focus attention on key aspects of cancer of care or cancer control.Data collected by a cancer registry are useful on several levels. The cancer registry records personal and medical information necessary for planning and evaluating the patient's case management. The registry data provide administrative information for facility planners, cancer committees, and practitioners. When the data are consolidated by population-based central registries, they are used by government and private agencies for developing and evaluating cancer control programs. Registries provide a rich source of data for investigative cancer research.Central registries including state registries, the National Cancer Data Base (ACDB), the North American Association of Central Cancer Registries (NAACCR), the Surveillance, Epidemiology and End Results (SEER) program, the National Program of Cancer Registries (NPCR) program, and other joint projects; collect data submitted electronically from multiple source registries. Without shared data-coding standards, the submitted data has to be reformatted and interpreted. Central registry administrators were among the first to realize the inconsistencies among contributing registries in data content, despite what seemed to be shared codes and procedures. Registries should obtain current information directly from the governing bodies that affect their operations.Standard Setters
The following three organizations were involved in the development of standard codes for describing the cancer itself: The World Health Organization (WHO), the American Cancer Society (ACS), and the American Joint Committee on Cancer (AJCC) developed standard codes for topography, morphology and extent of tumor spread.The following three organizations shaped standards for facility and population-based registries. The Commission on Cancer of the American College of Surgeons (CoC), defined the role of the facility registry in cancer management. The National Cancer Institute's Surveillance Epidemiology and End Results Program (SEER) developed procedures for central registry monitoring of data quality and the National Program of Cancer Registries (NPCR), administered by the Centers for Disease Control and Prevention, added incentives for population-based central registries to adhere to guidelines.The following two organizations overlap the others in time and purpose. Although all standard setting agencies run training programs, the National Cancer Registrars Association (NCRA) develops training programs specifically for registrars. The North American Association of Central Cancer Registries (NAACCR) promotes the development of standards shared by member central registries and the standard setters that sponsor it.Scope of Standards
Except as a record of individual case progress, all uses of cancer registry data involve compilations of data in statistical summaries. The interpretation of compiled data requires uniformity of data elements and consistent use of codes. Consequently, even if universal standards do not exist, most registries institute local guidelines to meet their immediate needs for data consistency.Interest in shared or uniform registry standards for data collection and management has grown with the increasingly varied use of registry data, stimulated by the adoption of computerized registry data systems. Contemporary standards for registry data and data management emphasize standardization of the data. That is, for items characteristically collected by cancer registries, the same codes are applied, coded by the same rules, and edited and updated according to the same guidelines. When standard rules for case inclusion or exclusion and standard grouping procedures are also followed, the resulting incidence, survival, and response rates have the same meaning no matter where they are produced. For registry data to be used optimally, uniform standards are necessary.Registry standards address diagnostic codes and general registry operations. The field of oncology data collection has continued to grow, especially since the advent of widespread computerization of registries. Clinical, epidemiological, and surveillance groups, as well as, organizations evaluating data quality, became increasingly interested in pooling or consolidating registry data. Data are pooled when records from multiple sources are combined into a single, large database; each record represents a unique case. Data that are compiled separately are compared for presentation in a single publication. When multiple records applying to a single case are included, the data are consolidated to form a single, more complete and accurate record.Data Sets
Data sets are lists of variables collected to meet the minimal requirements of the group's goals, often with an additional list of elements that are recommended for the most effective operation. Required data sets are not the same for all standard setters. For example, the underlying interest of the CoC is the quality of case management and medical care provided by the medical facility. Detailed information is collected on patients' prognostic factors, treatments and services provided, and short- and long-term outcomes. The NPCR data set was specified to meet cancer control goals of assessing timely diagnosis and reporting of cases, demographic factors affecting surveillance, first course of treatment, and mortality. SEER's data incorporate the goal of epidemiological research analysis and include items to indicate data quality. Many of the data needs for these and other programs are similar, and the required data sets naturally overlap.Most hospital-based (institution-based) registries are required to meet the standards of more than one organization and may also add specific variables to meet internal needs. Most registries in hospitals or other medical facilities are required to meet the data standards of both the CoC and a state central registry. The CoC data set, in turn, includes items necessary to code TNM categories and other items required by its member organizations. Most state registries, in turn, must meet data requirements set by SEER, NPCR, and state legislative mandate, in addition to those they setCode Categories
It is useful to distinguish between code categories (for example, race codes), and the codes assigned to them (01-99). Standard codes are necessary for reporting or exchanging data and are often more convenient to use internally. Standard categories must be retained in the registry structure, however, and conversion to and from standard codes must be built into routine computer operations. Because the application of codes must be similar for codes to indicate the same thing, it is not sufficient to convert nonstandard code categories into standard codes.There is a great need for consistent data standards. Data elements having the same intent should mean the same thing in every registry that collects them. When they do not, coders may need to code similar but not identical codes twice. Standard code categories, therefore, must meet multiple data goals. To and from standard codes must be built into routine computer operations.The standards specify not only what codes to apply to "known" categories but also distinguish categories such as "not available in the record," "not appropriate to this case," or "not collected by this registry." The format of the code — mixed or uppercase, left- or right-justified, numeric with leading blanks or numbers with a zero fill, blanks permitted or not — is also standardized. Rules for Code Assignment
Simply defining code categories does not ensure data consistency. Both technical and non-technical elements must follow rules for code category assignment. For example, how exactly does an abstractor select among multiple references to morphology in a record? When does the first course of therapy begin and end? Where does a transient live? The need for uniform rules for code assignment is well recognized by registries and standard setters, and more progress in this area is likely to be achieved over the next several years.Data Edits
Data edits test the logical effects of coding rules or natural relationships. For example, squamous cell carcinoma commonly develops in the lung but it is not expected to develop in the pleura. An automated edit could question or flag a case coded as squamous cell carcinoma of the pleura. Depending on how the edit is implemented by the registry software, it may prohibit saving that combination of codes, allow the registrar to set an override flag if necessary, or simply print an edit report.Data edited using varying data sets are not statistically comparable. This is an especially difficulty concept to grasp because it challenges a widely accepted axiom, "the more editing the better."The SEER program developed the first standard edits for registry data. Through the leadership of NAACCR, edit standards have been compiled for data elements within and across standard data sets. When edits are adopted, any updated or modified data in the registry should be re-edited. View the NAACCR Standard Edits for Cancer Registries, Volume IV.Case Consolidation
One of the major functions of a central cancer registry is to consolidate cancer case data from multiple reporting sources and facilities or institutions for the same patient (i.e., the reports are "consolidated" into one comprehensive case).The logic of case consolidation is closely related to both code category assignment and data editing. When data from multiple sources pertaining to the same person or case are combined, inevitable discrepancies between information on file and new data appear. Some discrepancies represent new information (for example, a more detailed morphology), some are erroneous such as a misspelled name. Consolidation rules determine which data inconsistencies can be resolved automatically and when to assign precedence of one category over another. Shared standards for case consolidation are likely to be developed in the coming years, as rules for code assignment evolve.Cases to be Covered by New or Changed Standards
Even though an important consideration in the use of standard code categories and procedures is continuity over time, introduction of new or revised codes is sometimes necessary. It is now accepted practice to specify a date of implementation for the new codes. Data collected with outdated codes are often no more useful than old data. For example, to be useful, the AJCC prognostic stage groups require updating as medical technologies advance. Old AJCC stage grouping lacks the prognostic value of the revised codes.Administrative Items
Standard administrative codes identify code version or flag exceptions to standard edits. Pooled data collected from multiple sources over a period of years require some method of identifying which codes were applied to those data. Sometimes codes are reviewed by splitting old code values into multiple new ones, and adding new categories, but often old codes take on new meaning. Both types of code change affect data distribution, and refined codes obviously affect code interpretation.Standard administrative items permit communication about the nature of the data in a form that can be interpreted by a computer program. Although administrative items are not an obvious component of a data set that serves the needs of any particular standard setter, they are valuable parts of shared or exchanged data. Some administrative items can be added by the registry computer program as cases are entered; others can be added automatically when data are written to exchange records. However, the registrar must manually add others, such as edit override flags.Data Management Procedures
Standards for data management procedures for hospitals (institution) and population-based registries have been defined by different standard setters. However, the scope of operations is similar: staff training and qualifications, case inclusion, case ascertainment, procedures for adding new cases to the permanent data set, rules for updating or changing data on file, follow-up, data exchange, and data analysis and publication.Hospital registry operational requirements are defined by the Standards of the Commission on Cancer, Volumes I, II, III, and IV. Specific standards are also defined by SEER and NPCR.For the most part, differences in data management standards reflect differences in registry operation and are not contradictory. For example, central registry case ascertainment standards require coverage of all facilities that care for cancer patients, whereas individual registries must check the records of all services in the facility in which cancer patients may be identified.However, registrars generally must comply with more than one standard for case inclusion. CoC specifications for facility registries identify the types of cases for which the facility, or its staff, have care responsibility. Many states require reporting of cases specifically excluded from CoC rules because central registries use this information to form a consolidated record for the patient from all sources. Hospitals occasionally collect data for cases not required by CoC or state/central registries. Benign brain tumors, pre-leukemic conditions, and similar diagnoses may be included by local standards.Review: Data Standards & Standard Setters
Here is what we have learned from Data Standards & Standard Setters:- Data collected by a cancer registry should be useful on several levels:
- The cancer registry records personal and medical information necessary for planning and evaluating the patient's case management.
- The registry data provide administrative information for facility planners, cancer committees, and practitioners.
- When the data are consolidated by population-based central registries, they are used by government and private agencies for developing and evaluating cancer control programs.
- Registries provide a rich source of data for investigative cancer research.
- The goals of standard setters help determine what registries collect and how the data are processed and ultimately used.
- The organizations of standard setters include WHO, ACS, AJCC, CoC, NCDB, SEER, NPCR, NCRA, UDSC.
- Data sets are lists of variables collected to meet the minimal requirements of the group's goals, often with an additional list of elements that are recommended for the most effective operation.
- Standard code categories must meet multiple data goals.
- Data edits test the logical effects of coding rules or natural relationships.
- Even though an important consideration in the use of standard code categories and procedures is continuous over time, introduction of new or revised codes is sometimes necessary.
- Standards for data management procedures for hospitals (institution) and population-based registries develop largely independently and have been defined by different standard setters.
Cancer As a Disease
The Cancer as a Disease module introduces you to the history of diagnosing and treating cancer, basic facts about the disease, how it is diagnosed and how we have been fighting cancer in our times.In this module you will learn how to:- Describe events in the history of diagnosing and treating cancer.
- Define the term cancer.
- Describe the methods of classifying and categorizing cancers.
- List known cancer risk factors of cancer.
- List different cancer types.
- Describe how cancer is diagnosed.
Cancer: A Historic Perspective
Since the earliest medical records were kept, cancer as a disease has been described in the history of medicine. The earliest known descriptions of cancer appear in seven papyri, discovered and deciphered late in the 19th century. They provided the first direct knowledge of Egyptian medical practice. Two of them, known as the "Edwin Smith" and "George Ebers" papyri, contain descriptions of cancer written around 1600 B.C., and are believed to date from sources as early as 2500 B.C. The Smith papyrus describes surgery, while the Ebers' papyrus outlines pharmacological, mechanical, and magical treatments.
Based on the information recorded on papyri and hieroglyphic inscriptions, ancient Egyptians were able to distinguish benign tumors from malignant tumors. They were also able to use different treatments, including surgery, and other various modes of medicine.
Following the decline of Egypt, the next chapters of medical and scientific history were written in Greece and Rome. The great doctors Hippocrates and Galen dominated medical thought for 1500 years. They lifted medicine out of the realms of magic, superstition, and religion. Hippocrates and Galen defined disease as a natural process, and based treatment on observation and experience. Cancers were identified, with warnings against treatment of the more severe forms. Hippocrates is credited with naming "cancer" as "karkinoma" (carcinoma) because a tumor looked like a "crab" ("karkinoma" is Greek for "crab") in that there is a central body to a tumor and the tumor extension appeared as the legs of the "crab".
After the fall of Rome, Constantinople became the intellectual storehouse of civilization. From there, in Arabic translations, classic Greek and Roman texts made their way back through Europe. The ancient teachings of Galen continued to inspire physicians in Constantinople, Cairo, Alexandria, Athens, and Antioch in a time when magic spells and myths dominated the West. Cancer continued to be explained as the result of an excess of black bile, curable only in its earliest stages.
In the modern world, science and surgery advanced as physicians returned to direct observation of the human body. However, the theory that cancer was caused by an excess of black bile continued to prevail in the 16th century. Cancer was considered incurable, although a wide variety of pastes containing arsenic were formulated to treat its manifestations. In the 17th century, the old theory of disease based on bodily humors was discarded when Gaspare Aselli discovered the vessels of the lymphatic system and suggested abnormalities of lymph as the primary cause of cancer.
Rejecting the 17th-century theory about the cause of cancer was the French physician Claude Gendron. He concluded that cancer arises locally as a hard, growing mass, untreatable with drugs, and must be removed with all its "filaments."
Two 18th-century French scientists, physician Jean Astruc and chemist Bernard Peyrilhe, conducted experiments to confirm or disprove hypotheses related to cancer. Their efforts, however absurd they seem in retrospect, established experimental oncology, the science of seeking better diagnosis, treatments and understanding of the causes of cancer. During this period, environmental cancers were reported, and hospitals specializing in cancer care were opened.
In the late 19th century, the development of better microscopes not only helped document and define disease-causing organisms, but also made possible the examination of cells and cellular activity. Study of cancer tissues and tumors revealed that cancercells were markedly different in appearance than normal cells of surrounding tissue or the cells from which they originated. Researchers began to focus on questions such as the origin of cells and the relationship of disease to the behavior of a cell. It was the invention of the microscope that revealed the cancer cell itself.
The early 20th century saw great strides made in understanding the structures, functions and chemistry of living organisms. Cancer research in cell culture, chemical carcinogens, diagnostic techniques and chemotherapy firmly established oncology as science. Researchers pursued different theories of the origin of cancer, subjecting their hypotheses to systematic experimentation. A viral cause of cancer in chickens was documented in 1911, and both chemical and physical carcinogens were conclusively identified. Chromosomal abnormalities were also investigated as possible causes of cancer.
In 1913, a need to combat rising public fear and ignorance concerning cancer led to two significant events: the publication of the first known article on cancer's warning signs in a popular woman's magazine, and formation of a nationwide organization dedicated to public education on cancer. Cancer, as a disease, was brought into the light of day.
In 1937, the U.S. Congress made the conquest of cancer a national goal with a unanimous vote to pass the National Cancer Institute Act. This Act created the National Cancer Institute, which was expected to break new theoretical ground by conducting its own research, promoting research in other institutions and coordinating cancer-related projects and activities. In 1971, President Richard M. Nixon signed the National Cancer Act, launching a National Cancer Program administered by the National Cancer Institute. Key events in the United States' national cancer policy legislative history, from 1937 to 1999 are available here.
Since its establishment, fundamental biomedical research supported by the National Cancer Institute has advanced the understanding of cancer. Using tools of molecular biology and molecular genetics, scientists are making great leaps in the discovery and mapping of links between chromosomes, the genes within, and cancer. In addition to traditional cancer therapies, potential solutions to the prevention and cure of cancer seem limited only by the imagination.
Review: Cancer: A Historic Perspective
Here is what we have learned from Cancer: A Historic Perspective:
- Ancient Egyptians first recorded cancer as a disease. From papyrus manuscripts and hieroglyphic inscriptions we learned that some 4500 years ago, attempts were already made by Egyptians to understand cancer and to treat the cancer patients, using surgery and magical treatments.
- In Greece and Rome, and throughout the Middle Ages, cancer was continuously regarded as a disease caused by an excess of black bile. While surgeries were carried out to treat cancer, doctors believed that the disease was curable only in its earliest stages and best left alone.
- In the 16th century, the theory that cancer was caused by an excess of black bile continued to prevail.
- During the 17th century, the old theory of disease based on bodily humors was discarded when Gaspare Aselli discovered the vessels of the lymphatic system and suggested abnormalities of lymph as the primary cause of cancer.
- Observations on environmental cancers were made in the 18th century. People started research on the connection between certain environments and cancer incidence patterns. With the first systematic experiments in cancer, oncology was born as a medical discipline.
- In the late 19th century, study of cancer tissues and tumors revealed that cancer cells were markedly different in appearance than normal cells of surrounding tissue.
- In the early 20th century, cancer research in cell culture, chemical carcinogens, diagnostic techniques and chemotherapy firmly established oncology as an experimental science.
- In 1937, the U.S. Congress passed the National Cancer Institute Act with a unanimous vote, creating the National Cancer Institute.
- In 1971, President Richard Nixon signed the National Cancer Act, launching a National Cancer Program administered by the National Cancer Institute.
What Is Cancer?
There are many texts and references that attempt to define cancer. The simplest definition is from the American Cancer Society (ACS). According to the ACS, cancer is a group of diseases characterized by uncontrolled growth and spread of abnormal cells. If the spread is not controlled, it can result in death.
(ACS). According to the ACS, cancer is a group of diseases characterized by uncontrolled growth and spread of abnormal cells. If the spread is not controlled, it can result in death.Characteristics of Cancer
Abnormality
Cells are the structural units of all living things. Each of us has trillions of cells, as does a growing tree. Cells make it possible for us to carry out all kinds of functions of life: the beating of the heart, breathing, digesting food, thinking, walking, and so on. However, all of these functions can only be carried out by normal healthy cells. Some cells stop functioning or behaving as they should, serving no useful purpose in the body at all, and become cancerous cells.
Uncontrollability
The most fundamental characteristic of cells is their ability to reproduce themselves. They do this simply by dividing: one cell becomes two, the two become four, and so on. The division of normal and healthy cells occurs in a regulated and systematic fashion. In most parts of the body, the cells continually divide and form new cells to supply the material for growth or to replace worn-out or injured cells. For example, when you cut your finger, certain cells divide rapidly until the tissue is healed and the skin is repaired. They will then go back to their normal rate of division. In contrast, cancer cells divide in a haphazard manner. The result is that they typically pile up into a non-structured mass or tumor.
Invasiveness
Sometimes tumors do not stay harmlessly in one place. They destroy the part of the body in which they originate and then spread to other parts where they start new growth and cause more destruction. This characteristic distinguishes cancer from benign growths, which remain in the part of the body in which they start. Although benign tumors may grow quite large and press on neighboring structures, they do not spread to other parts of the body. Frequently, they are completely enclosed in a protective capsule of tissue and they typically do not pose danger to human life like malignant tumors (cancer) do.
A Group of Diseases
Although cancer is often referred to as a single condition, it actually consists of more than 100 different diseases. These diseases are characterized by uncontrolled growth and spread of abnormal cells. Cancer can arise in many sites and behave differently depending on its organ of origin. Breast cancer, for example, has different characteristics than those of lung cancer. It is important to understand that cancer originating in one body organ takes its characteristics with it even if it spreads to another part of the body. For example, metastatic breast cancer in the lungs continues to behave like breast cancer when viewed under a microscope, and it continues to look like a cancer that originated in the breast.
Cancer Terms
Cancer, Neoplasia, Tumor, Neoplasm
The word cancer comes from the Latin (originally Greek) derived term for crab, because of the way a cancer adheres to any part that it seizes upon in an obstinate manner like the crab. Hippocrates first described cancer as having a central body with the tendency to reach out and spread like "the arms of a crab." Besides the popular, generic term "cancer" used by most people, there is another more technical term: neoplasia. Neoplasia (neo = new, plasia = tissue or cells) or neoplasm literally means new tissue in Greek. This indicates that cancers are actually new growths of cells in the body.
Another term for cancer is "malignant tumor." Tumor literally means "swelling" or "mass." In this case, it refers to a mass of non-structured new cells, which have no known purpose in the physiological function of the body.
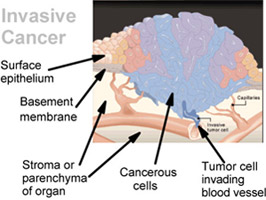
There are two general types of tumors: benign (non-cancerous) tumors and malignant (cancerous) tumors. A benign tumor is composed of cells that will not invade other unrelated tissues or organs of the body, although it may continue to grow in size abnormally. A malignant tumor is composed of cells that invade the basement membrane and invade or spread to other parts of the body. This occurs either by direct extension to neighboring organs and/or tissues or by metastasizing to distant sites by means of the vascular system (the blood stream), the lymphatic system, or by seeding or implantation of cancer cells in body cavities.
Terms such as "mass" and "lump" are used to describe any overgrowth of tissue. However, these terms may not necessarily mean that such growths contain cancer cells.
Types of Abnormal Cell Growth
In addition to neoplasia, there are several other terms referring to abnormal cell growth. These include the following:
Hyperplasia refers to an abnormal increase in the number of cells, which are in a normal component of that tissue and are arranged in a normal fashion with subsequent enlargement of the affected part. One example is thyroid hyperplasia, an enlargement of the thyroid gland caused by an abnormal rapid growth of the epithelial cells lining the follicles. Another example is: Guitar strumming leads to hyperplasia of the cells on the thumb (a callus is formed). The callus on the thumb is a hyperplastic growth.
Hypertrophy refers to an abnormal increase in the size of each cell, for example, the increase in cell size of cardiac muscle.
Metaplasia refers to the replacement of one mature cell type with another mature cell type: for example, squamous metaplasia of the respiratory columnar epithelium — as evidenced by the metaplastic cough of a smoker.
Dysplasia refers to the replacement of one mature cell type with a less mature cell type: for example, dysplasia of the cervix epithelium.
Hyperplasia, metaplasia, and dysplasia are reversible because they are results of a stimulus. Neoplasia is irreversible because it is autonomous.
Tumor Terminology Generalizations
Names of benign tumors usually end with "oma" regardless of their cell type. For example, a benign glandular tumor (epithelium tissue) is called adenoma and a benign bone tumor is called osteoma, while a malignant glandular tumor is called adenocarcinoma and a malignant bone tumor is called osteosarcoma.
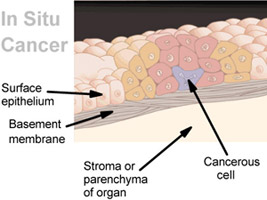
In addition to benign tumors, there are in situ tumors and invasive tumors. In situ tumors do not invade the basement membrane, whereas invasive tumors do invade the basement membrane.

No comments:
Post a Comment